
A newly released major study out of England, the Cass Review*, makes updated recommendations for treating kids with gender dysphoria. (Spoiler Alert: It’s not puberty blockers and hormones). The U.S. should heed the advice.
Gender dysphoria is a mental disorder that causes intense distress concerning the sex assigned at birth and extreme desire to become the other sex, or at least to look more like that other sex. Although the persistence of gender dysphoria from childhood and adolescence into adulthood has been low, less than one in five historically, immediate treatment with disabling drugs and later, disfiguring surgeries, are making it a lifelong chronic condition for many.
Even that one in five statistic is fairly unfounded because it’s been the Wild West out there with the domination of flippant gender affirming care practices as opposed to the comprehensive diagnosis and treatment of mental illness and disorders. Misinformation and misdiagnosis like claiming that kids were just born in the wrong bodies is common.
The study says that healthcare professionals should proceed with caution and avoid puberty blockers, hormone treatments and surgeries for kids. Instead, psychiatric or psychological therapies should be prescribed for mental healthcare. It turns out the age-old adage that medical treatment should first and foremost “Do No Harm” is particularly relevant here.
Meghan Murphy, a Substack writer and podcaster, says, “we need to scrap the entire concept of the ‘trans kid’ and the language of medicalized transgenderism. We should have done this from the getgo.” Indeed, there’s no time like the present to do just that.
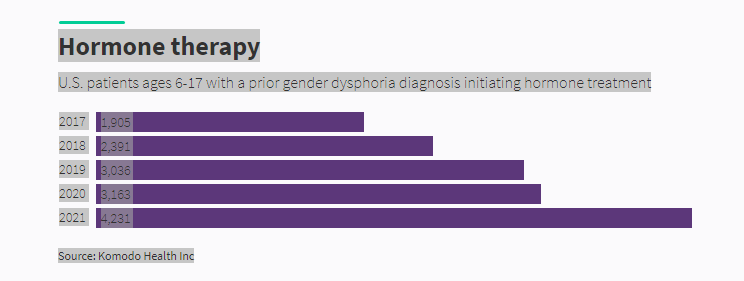
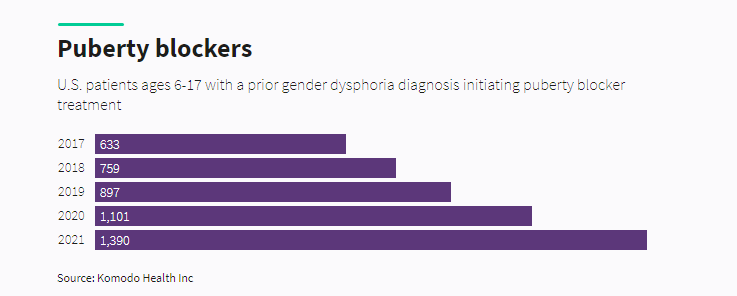
Gender dysphoria diagnoses have skyrocketed. Here’s what the occurrence trends look like from 2015 -2021:
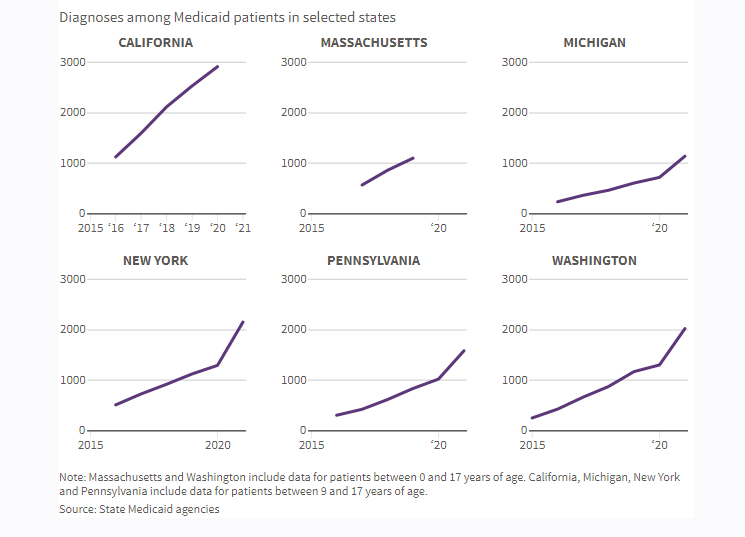
Although gender dysphoria historically afflicted males more, over the last decade or so gender dysphoria has become an epidemic affecting mostly adolescent girls. In this cohort it’s often called ROGD, Rapid Onset Gender Dysphoria. The reasons for this are not yet completely understood, but there are patterns.
The factors that seem to be triggering kids into diagnoses of gender dysphoria, especially amongst girls, include:
1. Autism. The child realizes that they don’t quite fit in socially, so they start believing that being a different gender would fix that. “6% of children with ASD (Autism Sprectrum Disorder) have gender dysphoria.” “From my perspective, the gender identity question has become one of the things that teens look for. Just like they have to figure out their own style of clothes, neurotypical and neurodiverse teens now have to define themselves. This is even more of a struggle for neurodiverse kids, who already feel different from others.”
2. Mental Illness. The child is not well and instead of remedying that psychotherapeutically, many therapists and doctors jump to the gender dysphoria diagnosis. Children with OCD are popping up as gender dysphoric, for instance. With the intensified public awareness and media coverage of issues concerning gender identity and gender incongruence, distinguishing true gender dysphoria or incongruence from the sexual obsessions of obsessive-compulsive disorder (OCD) is especially important. When you consider that many times children have one or two therapist or doctor visits, or even just a 15-minute conversation on the phone, before they’re prescribed puberty blockers and hormones, it’s particularly tragic.
3. Sexual Abuse. The child has experienced sexual abuse and the idea that changing genders would prevent further abuse contributes to gender dysphoria. “Seventy-three percent of TGAs (Transgender Adolescents) reported psychological abuse, 39% reported physical abuse, and 19% reported sexual abuse. Compared with heterosexual CGAs (Cisgender Adolescents), TGAs had higher odds of psychological abuse (odds ratio [OR] = 1.84), physical abuse (OR = 1.61), and sexual abuse (OR = 2.04). Within separate subgroup analyses, transgender males and nonbinary adolescents assigned female at birth had higher odds of reporting psychological abuse than CGAs.“
4. Pornography. The ubiquity of disturbing pornographic imagery scares kids, especially girls. How not? They don’t want to be the victim or recipient of any of the behaviors they see in the videos. They see an opportunity to change their gender as a prevention strategy. “Possible avenues of how pornographic content may increase the shame and fear of becoming a woman include the acquisition of misogynistic sexual scripts based on false assumptions on sexuality including the normalization of the violation of females as pleasurable for them, peer influence among female friendship groups, the susceptibility of our medical systems to “mass hysteria” phenomena, easier access of adults with sexually abusive intentions to youth through social media, sexual abuse and victim blaming on females, as well as the influence of pornography on mentalization capacities.“
5. Peer Interactions and Social Media. TikTok and other social media channels provide online spaces where TGNB (Transgender and Non-Binary) youth gather in communities. Although there’s little research to support or disclaim the effect of social media on TGNB youth, the closed “echo chambers” in these spaces could very well be exacerbating the disorder. The co-morbidity of Anorexia with Gender Dysphoria is common. Anorexia has a history of spreading like wildfire amongst females, though it also is widely seen amongst gays. “Some who experience gender dysphoria have the urge to alter their appearance through healthier means, like clothing choices or haircuts. However, some take it further by adopting a disordered diet. For some folks who are experiencing gender dysphoria, they may use the eating disorder—whether that’s restrictive eating or binge eating, or other disordered eating behaviors—to manipulate their body size and shape in order to alleviate that gender dysphoria,…”
6. Homosexuality. Sometimes a child senses that they’re not heterosexual and instead of just letting the child grow up to figure that out, the child is diagnosed with gender dysphoria. It’s also possible that some homophobic parents see transitioning as a way for their kid to look heterosexual while maintaining their homosexuality or that the children themselves are homophobic perhaps because of cultural or family issues. Without interventions of drugs and surgeries though, it’s entirely likely that those particular kids would grow up to be healthy homosexuals, lesbians, or bisexuals. This idea really upsets trans activists who at times appear to be on a mission to trans the world. If trans kids, adolescents, and young adults are attracted to the same sex they were before transitioning it does seem like a form of conversion therapy or a medicalized version of cross-dressing. I’ve seen this in my own extended family – lesbian before, lesbian after, but just a different physical appearance as a man. “The LGB community used to be a place where a butch woman could go to find acceptance for who she was. She could “act like a man” all she wanted and still be seen as a woman. However, now she is told that she really might be a man after all because she didn’t like pink dresses as a kid.”
7. Progressive Trans Ideology. Trans ideology is thrust upon kids everywhere it seems. Schools, the entertainment industry, media, social media, doctors, therapists, parents, and more are the “true believers” when it comes to declaring kids trans and pushing the gender affirming care on kids. The rush to accommodate or affirm gender dysphoria rather than treat it as a disorder is tragic. Journalist Michael Shellenberger recently exposed what a sham WPATH, the World Professional Association for Transgender Health, is. This video shows WPATH “professionals” casually commenting on getting informed consent from children for treatments that will likely make them sterile, sexually dysfunctional, and possibly cognitively impaired as a result of gender affirming care.
To be clear, homosexuality, lesbianism, and bisexuality are not mental disorders that call for treatment. Additionally, they are not transient or connected to any of the factors listed above. The occurrence is about one in ten across the globe and throughout history. Not so transsexuality, an anomaly of a mental disorder which historically occurred about once in 3000 people… that is until the very recent past.
Personally, I’ve come to the conclusion that I’m “somewhat over the rainbow” because while I support the LGB, I have extreme skepticism of every letter and symbol after that, i.e. TQIA+. This is not to say I don’t have compassion for people suffering from gender dysphoria and other mental illnesses and disorders or even people caught up in fetishes or sexual obsessions, it’s just that these should be treated not affirmed. As Bill Maher quips, if a child wants to be a pirate, we don’t remove an eye.
Trans proponents argue that it’s not something to be fixed, but further scrutiny indicates that it is and that affirming care for gender dysphoric children lacks a scientific basis as per the 388-page Cass Review that was recently released. The increasingly large number of children diagnosed with gender dysphoria deserves pause, scrutiny, and a full-blown scientific investigation which is why the report was written.
Recommendations from the report suggest extreme caution and that children should not be ushered into “gender affirming care” with instant access to drugs and later surgeries, they need sufficient psychiatric or psychological care. Remember that most gender dysphoria in children is transient. In this case, therapeutic care with a heavy dose of patience may indeed allow for the disorder to pass or a more accurate diagnosis of the problem to happen. That, unfortunately, has not been allowed.
Puberty blockers and hormone treatments are not harmless and reversible contrary to conventional wisdom, let alone surgeries that often follow childhood. Cognitive issues, weakening of bones, sterilization, sexual dysfunction, and no chance to experience orgasms in the future are just some of the possible side effects. Our sources for information and practice have not kept up with the science. The real sad part is that it’s uncommon for kids with gender dysphoria to continue to have it after adolescence into adulthood. It’s almost always transient. This is why so-called “gender affirming care” is so tragic and is in many ways a horrifying kind of conversion therapy. We must do no harm to children.
In Washington State, a 13-year-old with gender dysphoria can decide for themselves to take puberty blockers and hormones even though their brains don’t fully develop until 25. They can go to school, a therapist, or a doctor and assume new pronouns, get connected to “gender affirming care” and quickly begin treatments that cause irreversible damage. They don’t even need their parents’ permission or even their knowledge of what’s going on. I get that there are parents who are the root of the psychological problems that the kid is experiencing, but without sensible and science-based guardrails, the gender dysphoria “cure” is worse than the ill.
It gets worse. Families are now ineligible to foster children in Washington State if they don’t agree to gender affirming care for the gender dysphoric kids. If you review that list earlier in this post about the conditions that tend to be associated with gender dysphoria, foster kids are typically dealing with many of those things. Drugs and surgeries are not the answer for children, psychotherapy is.
Although the United States is late to recognize that, other countries have come to their sense. “The U.K. is not the only nation to make major changes to its approach to care for transgender-identifying minors. In recent years, national health authorities in Sweden, Norway, Finland, and France have also taken a second look at the gender-affirming care model and changed course.” This has happened because of a complete lack of evidence that drugs and surgeries are appropriate for treating gender dysphoria in kids and a lot of evidence that not only are they unhelpful, but that they likely cause irreversible damage. “Health care should not provide interventions that we do not know to be safe and beneficial,” Mikael Landén, a professor and chief physician at the University of Gothenburg in Sweden and co-author of the report, wrote in an email. “From the lack of evidence follows that a conservative approach is warranted.”
Now that longitudinal studies prove that as per the Cass Review and other current research, many countries are adjusting their protocols appropriately. That change in protocols can’t come soon enough to the United States.
Sources:
NOTE: Some sources that have informed this post are below, others are linked within the content.
“Britain Is Leaving the U.S. Gender-Medicine Debate Behind” by Helen Lewis, The Atlantic, April 15, 2024
“The Cass Review damns England’s youth-gender services”, The Economist, April 10, 2024
“Independent review of gender identity services for children and young people: Final report”, by Dr Hilary Cass, April 9, 2024
“What does Cass review mean for future of gender care?”, Richard Windsor, The Week, April 10, 2024
“The WPATH Files”, Michael Shellenberger, March 5, 2024
Information from Microsoft Copilot (Artificial Intelligence):
*The Cass Review, also known as the Independent Review of Gender Identity Services for Children and Young People, was commissioned by NHS England and NHS Improvement in 2020. It was led by Dr. Hilary Cass, a retired consultant paediatrician and former President of the Royal College of Paediatrics and Child Health1. The review focused on gender services for children and young people, including those with gender dysphoria and those identifying as transgender.
The final report of the Cass Review was published on April 10, 20241. It included several systematic reviews of scientific literature carried out by the University of York, covering various aspects related to gender identity services:
- Patient cohort
- Service pathways
- International guidelines
- Social transitioning
- Puberty blockers
- Hormone treatments
The Cass Review found that the evidence for the use of puberty blockers and cross-sex hormones as treatment for gender dysphoria is quite weak. Specifically:
- For puberty blockers, there is no evidence that they improve body image or dysphoria, and limited evidence for positive mental health outcomes. Additionally, their use is associated with significant loss in bone density, and brain maturation may be disrupted, potentially impacting decision-making abilities and long-term neuropsychological consequences.
- Regarding cross-sex hormones, there is a lack of high-quality research assessing outcomes in adolescents with gender dysphoria2.
The review also addressed the issue of social transition, emphasizing its consequences, especially for younger children. While U.K. schools are prepared to socially transition a child without informing parents, the Cass Review asserts that social transition is significant and should not overshadow other issues such as poor mental health2.
Overall, the Cass Review’s findings have had a substantial impact on gender medicine discussions and practices, both in the U.K. and internationally2.
Important Links from Colin Wright:
the LGBT Courage Coalition, the Society for Evidence-Based Gender Medicine, Genspect, Do No Harm, and Therapy First.